#뇌전증 (EPILEPSY), 체내칸나비노이드(ENDOCANNABINOIDS), 식물칸나비노이드(PHYTOCANNABINOIDS)
CBD와 다른 여러 가지 칸나비스 성분은 발작 장애 환자를 도울 수 있으며, 때로는 CBD를 기존 항-뇌전증약과 병용하는 것이 가장 좋습니다.
Cannabidiol and several other cannabis components can help patients with seizure disorders, and sometimes it's best to combine CBD with conventional anti-epileptic meds.
BY STACEY KERR, M.D. ON NOVEMBER 25, 2017
Highlights:
500만명 이상의 미국인이 뇌전증에 시달립니다.
More than 5 million Americans suffer from epilepsy.
CBD는 발작장애아 등 많은 환자들을 돕고 있습니다.
CBD is helping many patients, including children with seizure disorders.
종종 환자는 자기 병에 대한 최상의 치료 방법을 찾기 위해 여러 칸나비스 제품을 시험해야 합니다.
Oftentimes, patients must experiment with different cannabis products to find the best remedy for their condition.

뇌전증 관리를 위한 칸나비스 사용에 대한 약속이 있습니다
There's promise in the use of cannabis to manage epilepsy
뇌전증은 복잡한 의료, 경제, 사회 문제로 2013년 인구통계에 의한 최소 510만 명 미국인에게 영향을 미칩니다.
Epilepsy is a complex medical, economic, and social issue that affects at least 5.1 million of the US population by 2013 population reports.
하와이에는 약 1만 5천명의 발작장애 환자가 있습니다.
In Hawaii, there are an estimated 15,000 patients with seizure disorders.
미국에서 뇌전증의 직간접 비용은 매년 155억 달러로 추정됩니다.
The total indirect and direct cost of epilepsy in the United States is estimated to be $15.5 billion yearly. 1, 2
강아지건강 전문
www.dopza.com
발작장애 환자나 가족의 경우, 발작 유형과 빈도 그리고 항-발작약의 영향(치료효과와 부작용)에 따라 생명이 제한되고, 매우 복잡할 수 있습니다.
For the individuals and families of those patients with seizure disorders, life can be limited and extremely complicated depending on the type and frequency of seizures and on the effects of anti-seizure medications, both therapeutic and undesirable.
발작은 뇌의 일부가 지나치게 흥분되거나 뇌 신경이 비정상적으로 발화 fire 할 때 발생합니다.
Seizures occur when a part of the brain becomes overly excited or when nerves in the brain begin to fire in an abnormal way.
흥분성 신호 excitatory signals 방아쇠와 억제신호간 급격한 불균형으로 흥분력 excitatory forces 이 발생됩니다.
An abrupt imbalance between the triggers of excitatory signals and inhibitory signals causes the excitatory forces to take over.
이 자극은 주변 세포로 전파되어 모두 같은 비정상적 방식으로 발사 fire 하기 시작합니다.
This excitation then spreads to surrounding cells which all start firing in the same abnormal way.
다양한 잠재적 공격으로 인한, 신경세포의 흥분 증가 또는 신경세포의 억제 감소로 발작이 일어날 수 있습니다.
Increased excitation of nerve cells, or decreased inhibition of nerve cells due to a variety of potential insults can lead to a seizure.
균형 또는 항상성이 혼란스러워집니다.
Balance, or homeostasis, is disrupted.
대부분의 뇌전증 환자는 발작 원인이 알려져 있지 않습니다.
Most epileptics have no known cause for their seizures.
외상 trauma, 감염 infections, 선천적 신진대사 오류, 마약(또는 마약 중단), 유전병 등 수많은 사소한 원인도 밝혀졌습니다.
The minority have numerous identified causes that include trauma, infections, inborn metabolic errors, drugs (or withdrawal from drugs), and inherited conditions.

기존 치료방법
Conventional treatment
발작의 근본 원인에 대한 치료법이 없으며, 두부 외상 후 발작 발병을 확실히 예방하는 치료법은 없습니다.
There are no treatments for the underlying causes of seizures, and no treatments to reliably prevent the development of seizures after head traumas.
발작 강도 또는 빈도를 제한하는 약물만 있으며, 이러한 약물도 항상 효과가 있는 것은 아닙니다.
There are only medications to limit the seizure intensity or frequency, and these medications are not always effective.
사실, 뇌전증 환자의 3분의 1은 적절히 처방된 항-뇌전증약(AEDs)을 2가지 이상 사용하고 견딘 후에도 발작에서 벗어나지 못합니다.3
In fact, a third of epileptic patients fail to become seizure free even after trying and tolerating two or more appropriately prescribed anti-epileptic drugs (AEDs).3
지난 수십 년 동안 20가지 이상의 새로운 발작 약품이 개발되었지만, 억제되지 않는 발작 환자 비율은 희망이나 기대만큼 많이 변하지 않았습니다.
More than 20 new seizure medications have been developed over the past few decades, but the percentage of patients with uncontrolled seizures has not changed as much as we would hope or expect.
AED에 내성있는 환자는 뇌전증으로 인한 합병증 및 급사 위험이 더 높습니다.
Patients who are resistant to AEDs have a higher risk of complications and sudden death due to epilepsy.
여러 AED가 필요한 경우에도 심각한 부작용이 증가합니다.
The need for multiple AEDs also increases the occurrence of significant side effects.
더 좋고, 더 안전한, 효과적 치료의 필요성은 분명합니다.
The need for better, safer, and more effective treatment is clear.
칸나비노이드 전문
www.dopza.com
안전 성분
Safety profile
칸나비스는 뇌간 brainstem에 칸나비노이드 수용체가 없어 사망자가 발생하지 않는 안전한 약제입니다.
Cannabis is a safe medication with no incidence of fatalities due to the lack of cannabinoid receptors in the brainstem.
발작 조절을 위해 칸나비스를 사용하는 환자들 사이에 보고된 가장 일반적 부작용은 피로감, 식욕감소, 졸림 현상이며, 칸나비스 투여가 중단되면 해결됩니다.
The most common side effects reported among patients using cannabis for seizure control are fatigue, decreased appetite, and somnolence, all of which resolve when cannabis is discontinued.
AED는 상당한 부작용이 있을 수 있으며, 칸나비스와 달리 일부는 치명적일 수 있습니다.
AEDs can have significant side effects, and contrary to cannabis some of these can be fatal.
칸나비노이드는 간에서 시토크롬 P-450 체계에 의해 주로 대사되기 때문에, 칸나비스를 AED와 함께 사용할 때는 약물-약물 상호작용이 있음을 주지하는 것이 중요합니다.
It is important to note that there are some drug-drug interactions when using cannabis with AEDs because cannabinoids are primarily metabolized by the Cytochrome P-450 system in the liver.
이들 효소에 대한 경쟁은 AED의 혈청 수준에 영향을 줄 수 있으므로, 처방된 AED와 함께 칸나비스를 사용하는 환자는 모니터링해서 용량을 조정해야 할 필요도 있을 수 있습니다.
Competition for these enzymes can affect the serum levels of AEDs, so patients using cannabis in addition to prescribed AEDs should be monitored, and dosage adjustments may be needed.

뇌전증의 체내칸나비노이드 체계(ECS)
The endocannabinoid system in epilepsy
ECS의 임무는 항상성을 유지하는 것이므로 수세기 동안 발작 조절에 도움이 되는 칸나비스가 사용된 것은 놀라운 일이 아닙니다.
The job of the endocannabinoid system is to maintain homeostasis, so it is no surprise that cannabis has been used to help control seizures for centuries.
쥐에 대한 잘 고안된 연구에 따르면 ECS는 발작 장애에 대한 뇌 반응의 중요한 부분입니다.
Well-designed studies on rats have shown that the endocannabinoid system is a significant part of the brain’s response to seizure disorders.
칸나비노이드 수용체가 특히 중추신경계에 밀집되어 있다는 것은 잘 알려져 있으며, 칸나비스의 발작 억제 효과를 설명하는 모든 메커니즘이 완전 이해되지는 못했지만 이론은 갖고 있습니다.
We know that cannabinoid receptors are particularly dense in the central nervous system, and while we do not yet completely understand all the mechanisms that explain the anti-seizure effects of cannabis, we do have theories.
감정과 기억 암호를 처리하는 뇌의 일부인 해마 hippocampus에는 칸나비노이드 수용체가 있습니다.
There are cannabinoid receptors in the hippocampus, that part of the brain that handles emotions and memory encoding.
해마 세포의 비정상적 변화는, 가장 흔한 형태 중 하나인 내측 측두엽 medial temporal lobe 뇌전증의 원인입니다.
Abnormal changes in cells in the hippocampus are a cause of medial temporal lobe epilepsy, which is one of the most common forms.
이런 유형의 뇌전증에서, 해마 세포는 발작을 유발하는 흥분성 피드백 루프를 생성합니다.
In this type of epilepsy, hippocampal cells create an excitatory feedback loop that causes seizures.
동물과 인간연구에 따르면 칸나비노이드는 정상 해마세포를 보호하는 것으로 보이며 비정상세포를 덜 활동적으로 만들 수 있습니다.4
Animal and human studies show that cannabinoids seem to be protective of the normal hippocampal cells, and may make the abnormal cells less active.4
급성 발작 동물에서, 체내칸나비노이드 2-AG가 대조군에 비해 유의하게 증가했습니다.
In acutely seizing animals, the endocannabinoid 2-AG was significantly increased compared to controls.
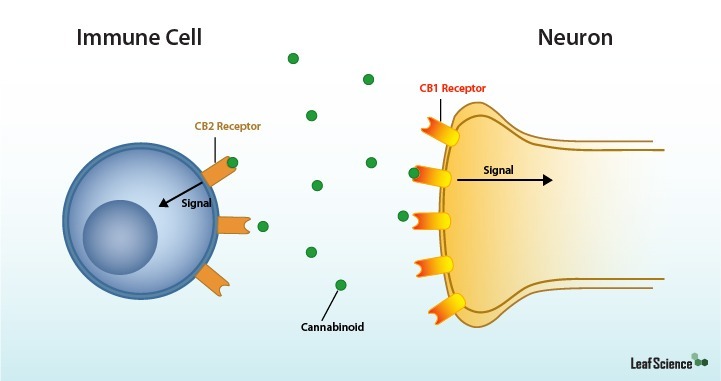
아난다마이드와 2-AG 수준을 시험한 결과, 발작이 일어날 때 요구에 따라 2가지가 합성되어 CB1 수용체를 활성화시키는 것을 보았습니다.
By testing the levels of both anandamide and 2-AG we have seen that both are synthesized on demand when seizures occur, thus activating the CB1 receptors.
또한 뇌전증 동물에서 CB1 수용체 발현이 유의하게 증가하는 것으로 나타나서, 연장된 아마도 영구적인 수용체 증가가 있는 것으로 보입니다.
It also appears that there is a significant increase in CB1 receptor expression in epileptic animals, a receptor increase that is prolonged and probably permanent.
칸나비노이드 전문
www.dopza.com
최근 몇 년 동안 동물 모델과 인간의 임상 관찰에 대한 연구가 뇌전증 조절에의 칸나비스 사용에 대한 관심을 다시 불러 일으켰습니다.
In more recent years research on animal models and human clinical observations have rekindled interest in using cannabis to control epilepsy.
칸나비노이드는 중추신경계의 글루타메이트 glutamate 합성을 감소시켜 염증과 발작을 감소시킵니다.6
Cannabinoids decrease glutamate synthesis throughout the central nervous system, which in turn decreases inflammation and seizure activity.6
메커니즘에 관계없이 사람의 임상 관찰은 칸나비스를 단독으로 사용하거나 보조 요법으로 사용하는 데 유망합니다.
Regardless of the mechanism, human clinical observations are promising for the use of cannabis as an anti-epileptic medication, either alone or as adjunctive therapy.
약으로서의 특정 칸나비노이드
Specific cannabinoids as medicine
증거는 식물 전체 사용이 단 하나의 격리 성분보다 효과적이라는 것을 계속 지적하는데, 아마도 동반 효과 때문입니다.
The evidence continues to indicate that whole-plant usage is more effective than any single isolated constituent, perhaps due to the entourage effect.
칸나비스에는 많은 칸나비노이드가 들어 있으며, THC와 CBD는 80가지 이상의 가능성 중 2가지입니다.
Cannabis contains many cannabinoids, THC and CBD being only two of over 80 possibles.
또한, 칸나비스 식물에게 향기를 주는 의학적 활성 화합물인 테르펜(terpenes)을 함유하고 있습니다.
In addition, the plant contains terpenes which are medically active chemicals that give the plant its fragrance.
이러한 성분을 결합하면 단일 칸나비노이드와 함께 병의 부작용을 줄일 수 있으며 발작 조절에 더 효과적일 수 있습니다.
Combining these constituents can decrease side effects from any single cannabinoid and together, and may be more effective in controlling seizures.7
특정 유형의 발작에 가장 적합한 조합이 무엇인지 아직 알지 못하지만 증거는 더 많은 연구 노력을 격려하기에 충분합니다.
We do not yet know what the best combination is for any specific type of seizure but the evidence is strong enough to encourage more research efforts for answers.
CBD는 발작 장애를 치료하는 주된 칸나비노이드입니까?
Is CBD the primary cannabinoid that treats seizure disorders?
심각한 증상의 어린이들에 대한 최근 보고를 고려한다면 그렇게 생각됩니다.
It seems so if you consider the recent reports of use in severely affected children.
CBD는 확실히 중요한 역할을 하지만, 유일한 분자는 아닙니다.
CBD is certainly a major player, but not the only one.
CBD는 많은 사람들에게 임상적으로 항-경련제로 입증되어 왔으며, 최악의 경우 소수 뇌전증 환자에게는 효능이 없었습니다.
CBD has been clinically proven as an anticonvulsant for many and at worst, for a minority of patients with epilepsy, it gave no benefit.
CBD의 항경련효과는 아마도 유익한 활동의 조합 때문일 것입니다.
Its anti-convulsive effects are probably due to a combination of beneficial activities.
CBD는 NMDA 수용체(AED Felbamate와 유사)를 차단하고, GABA 수용체를 강화합니다(phenobarbital, Depakote와 유사).
CBD blocks NMDA receptors (similar to the AED Felbamate) and enhances GABA receptors (similar to phenobarbital and Depakote).
CBD는 이온 채널(Dilantin, Keppra와 유사)을 안정화시키고, 항-염증제 역할을 하며, 신경보호제 역할을 합니다8.
It stabilizes ion channels (similar to Dilantin and Keppra), acts as an anti-inflammatory, and also as a neuroprotectant.8
칸나비노이드 전문
www.dopza.com
복용법
Dosing
칸나비스는 2상 복용-반응을 나타내어 더 많이 복용한다고 항상 더 좋거나 더 효과적이지는 않다는 것을 의미합니다.
Cannabis has a biphasic dose-response, meaning that more is not always better or more effective.
성인 복용량은 0.02mg/kg/day이지만, Epidiolex(GW Pharmaceuticals가 정제한 CBD 제품)에 대한 임상실험은 2-50mg/kg/day의 범위를 테스트했습니다.
Dosing for adults has been noted at amounts as small as .02 mg cannabinoids/kg/day, but the clinical trials done on Epidiolex (a purified CBD product made by GW Pharmaceuticals) tested a range of 2-50mg/kg/day.
발작에 대한 칸나비스 복용약은 여전히 진화하는 과학이지만, 난치성 발작을 치료하는 경험있는 의사는 다음 지침을 제공합니다.
While dosing cannabis for seizures is still an evolving science, an experienced physician treating children for intractable seizures shares the following guidelines.
첫째, CBD 오일을 시작하기 전에 EEG를 기록한 다음, 개선을 보이면 1-3개월 후에 반복합니다.
First, an EEG is recorded prior to starting CBD oil and then repeated at 1-3 months if the child is showing improvement.
이들 복용량은 아이의 결과에 따라 1-2주마다 증가합니다.
These doses are increased every 1-2 weeks depending on the child’s results.
많은 환자의 치료 범위가 4-9mg/kg/day 사이인 것으로 나타났습니다.
She notes that the therapeutic range for many patients appears to be between 4-9 mg/kg/day.
발작 빈도가 감소함에 따라 AED도 천천히 줄일 수 있습니다.10
As the seizures decrease in frequency, it is possible that the AEDs can be slowly weaned.10
뇌전증 치료를 위한 칸나비스 사용에 관하여, 메인주, 워싱턴주, 캘리포니아주의 경험있는 3명의 의사가 최신 자료를 제공합니다.
The latest publication on the use of cannabis for the treatment of epilepsy comes from three physicians with experience in the states of Maine,
Washington, and California.
272명 환자 중 14%는 칸나비스가 발작을 줄이는데 효과적이지 않았으며, 15%는 발작이 1-25% 감소했고, 28%는 76-99%의 감소를 경험했으며, 10%는 완전한 임상 반응을 보였습니다.
Of their 272 combined patients, fourteen percent found cannabis to be ineffective at reducing seizures, fifteen percent experienced a 1-25% reduction in seizures, twenty-eight percent experienced a 76-99% reduction, and ten percent had a complete clinical response.
CBD made the difference
Sam은 4살 때, 첫 번째 간대성근경련 myoclonic 발작이 있었고, myoclonic 결핍 발작으로 진행되었습니다.
When Sam was 4, he had his first myoclonic seizure, and those progressed to myoclonic absence seizures.
Sam은 바닥에 떨어져 경련을 일으키지 않았습니다.
Sam did not fall to the floor and twitch.
대신, 하루에 100번, 한 번에 20-30초 동안 의식을 잃었습니다.
Instead, sometimes 100 times a day, he lost consciousness for 20-30 seconds at a time.
멈추고, 빤히 쳐다보며, 머리는 리드미컬하게 튕겨져 나갔고 모든 것이 끝났습니다.
He stopped, stared vacantly, his head bobbed rhythmically and then it would all be over.
심지어 발작을 눈치채지 못했고, 발작이 오면 주위의 모든 것이 약간 옮겨졌을 뿐입니다.
He didn’t even notice these seizures, only that when he would come to, everything around him had shifted slightly.
하지만 그것이 정상 삶을 하지 못하게 하였습니다:
완전한 대화를 하고, 학교에서 배우고, 스포츠에 참여하는 것이 어려웠습니다.
But it kept him from a normal life: having full conversations, from learning in school, and from participating in sports.
Sam은 정맥내 면역글로불린(immunoglobulin)과 케톤 생성 식단(ketogenic diet) 등 거의 20여 가지 치료법을 시도했습니다.
Sam had tried almost two-dozen treatments including intravenous immunoglobulin and a ketogenic diet.
이 중 일부는 효과적이었고, 걱정스러운 부작용(손떨림, 두드러기, 좀비 의식 등)이 있었고 또는 잠시 후 작업을 중단하기도 했습니다.
Few of these were effective, and those that were either had worrisome side effects (hand tremors, hives, zombie consciousness, etc.) or they quit working after a short while.
11살이 되던 해 그는 corticosteroids를 엄청 먹었는데 - 아무런 효능이 없는 것으로 밝혀졌지만 부작용은 엄청났습니다.
By the time he was 11, he was on massive doses of corticosteroids – the only thing they’d found that made any difference – but the side effects were devastating.
두 번 입원했고 3개 주에서 6명의 신경전문의 치료를 받았습니다.
He’d been hospitalized twice and seen six neurologists in three states.
그런 다음 최후수단으로 부모님은 CBD 시도를 결정했습니다.
Then, as a last resort, his parents decided to try CBD.
그 결과는 심오했지만 쉬운 일은 아니었다고 아버지는 말했습니다.
The effects were profound, but the road was “not a straight line,” to quote his father.
CBD는 즉각적으로 도움을 주었습니다 - 발작율이 목요일 68에서 다음 월요일에는 6으로 떨어졌습니다.
CBD had immediately helped – dropping the seizure rate from 68 on a Thursday to 6 on the following Monday.
CBD 시작한 지 몇 년 후, Sam은 CBD 1000mg에 대해 하루에 0번에서 5번까지 발작이 있었고, 다른 발작약은 복용하지 않았습니다.
A few years after starting the CBD, Sam was down to between 0 and 5 seizures a day on 1000mg of CBD and taking no other seizure medications.
그런 다음, 그는 최초의 일반화된 tonic-clonic 발작이 있었습니다.
Then, he had his first-ever generalized tonic-clonic seizure.
3주 후 다른 병이 생겼는데, Depakote가 처방에 추가되었습니다.
Three weeks later he had another, so Depakote was added to his regimen.
Depakote는 효능이 작동했습니다.
The Depakote worked.
Sam은 현재 15살이며 발작없이 15개월을 보냈습니다.
Sam is now 15 years old and has had 15 months without a seizure.
부모에게 이것은 기복이며 기적입니다.
To his parents, this is a relief and a miracle.
하루 875mg의 Depakote와 250mg의 CBD를 1일 2회 복용하고 있습니다.
He is taking 875mg of Depakote a day, and 250mg of CBD twice a day.
칸나비노이드 전문
www.dopza.com
이제는 스포츠, 플라이 낚시, 암벽 등반에서 활약하는 Sam은 정상적 소년이 되었습니다.
Now active in sports, fly fishing and rock climbing, Sam gets to be a normal boy.
분명히, 뇌전증을 관리하는데 칸나비스 사용의 약속이 있으며 아직도 연구가 더 필요합니다.
Clearly, there is promise in the use of cannabis to manage epilepsy and still much to learn.
Stacey Kerr MD is a teacher, physician, and author living and working in Northern California. Dr. Kerr was in private practice until she decided to write and educate full-time. After several years working with the Society of Cannabis Clinicians, and co-developing the first comprehensive online course in cannabinoid medicine, she is now serving as the Medical Director for Hawaiian Ethos, an evidence-based cannabis company on the Big Island of Hawaii.
This article was reprinted by Project CBD with permission. It may not be reproduced in any form without approval from the source.
1. (cdc.gov/epilepsy)
2. (http://www.epilepsy.com/hawaii)
3. Kwan P. Brodie MJ. Early identification of refractory epilepsy. N Engl J Med 2000;342(5):314-9
4. Gloss, Vickrey. Cannabinoids for Epilepsy. The Cochrane Library, 2012
5. Wallace M.J. et al. The Endogenous Cannabinoid System Regulates Seizure Frequency and Duration in a Model of Temporal Lobe Epilepsy, Journal of Pharmacology and Experimental Therapeutics, Vol. 307:129–137, 2003
6. Devinsky et al. Cannabidiol: Pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders. Epilepsia, 55(6):791–802, 2014
7. Rosenberg EC, Tsien RW, Whalley BJ, Devinsky O. Cannabinoids and epilepsy. Neurotherapeutics. 2015;12:747–768
8. Jones NA, et al. 2010. Cannabidiol displays anti-epileptiform and anti-seizure properties in vitro and in vivo. Journal of Pharmacology and Experimental Therapeutics 332(2):569-577
9. Sulak D, et al. The current status of artisanal cannabis for the treatment of epilepsy in the United States, Epilepsy Behav (2017), http://dx.doi.org/10.1016/j.yebeh.2016.12.032
10. Hill et al, Cannabidivarin is Anticonvulsant in Mouse and Rat, Br J Pharmacol. 2012 Dec;167(8):1629-42. doi: 10.1111/j.1476-5381.2012.02207.x.
11. Elisabetsky E, Brum LS, Souza DO. Anticonvulsant properties of linalool in glutamate related seizure models. Phytomedicine 1999;6(2):107-13
12. Bonnie Goldstein MD. https://www.theroc.us/goldstein.pdf
댓글